Dwayne Wade, Knee Pain and how it isn't as easy as you want it to be
Dwayne Wade’s collision with Chicago Bulls Guard Jimmy Butler during game four of the playoffs has the kneecap itself in the news, mostly because he can be seen on the sidelines pushing his kneecap into different places, trying to find a position that reduces his knee pain, as well as trying to keep said kneecap in that sweet, elusive spot with tape, braces, neoprene sleeves and rubber cement (OK, maybe not rubber cement). And it may have you thinking about your own kneecap, since there is a good chance that at some point you have had pain around that area yourself, and if not you most certainly know someone who has.
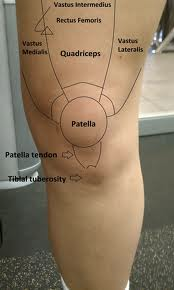
The kneecap (formally known as the patella; we’re inclusive here, so I’ll just keep saying kneecap) sits just in front of the bottom of the thigh bone. The fancy-schmancy name for the joint formed between these bones is the patellofemoral joint, and since I can’t think of a lay term, we’ll just keep saying patellofemoral joint. The kneecap itself is imbedded in the tendon connecting the large quadriceps muscles to the tibia and is important functionally because it increases the mechanical advantage of the quadriceps, effectively increasing their strength by about 30%.

It’s estimated that about 25% of injuries to the knee are related to the kneecap itself. For those people who do not have a sudden, traumatic injury--Dwayne Wade, who bruised his kneecap excepted--that number is much higher. In our practice we see a great deal of runners, and many of their complaints are of pain over and around the kneecap. We also see a lot of folks that are older and less active, the people who are trying to avoid knee replacement surgery. Where is their pain? The front of the kneecap. So, how is it treated?
One of the first steps that we take is to go over ways to decrease the stresses on the area around the kneecap. First off, we need to find alternatives to aggravating activities. Common aggravating factors of knee pain include walking down stairs. Look for an elevator first. If there is a railing to help you lower your body under control, or if you can go backwards without any risk of losing your balance, or if you can step down with only your painful leg (putting two feet on each step), try one of those alternatives. Of course, this only works if it is more important for you to get better than the conceit that strangers care how you descend staircases.
Prolonged sitting is another aggravating factor for pain in the kneecap. The answer to this is to simply stand up more frequently. If you have a desk job, stand up every 10 minutes or so. You can set a timer, or find a trigger: stand up every time the phone rings, you get an email, or your co-worker says something that annoys you. When you are not standing, try keeping your leg in a straighter position than normal. Sometimes it helps to put a stool or phone book, if they still make those, under your foot.

Running is the big one of course. As my one of my biomechanics instructors in PT school always said “try telling a runner to stop running.” Personally, I would never do that, but again, it is important to reduce the stresses on that kneecap. In cases where a race is not right around the corner, I do advocate a reduction in training volume. When that is not a good option, a switch to cross-training can be helpful, with just enough distance running at race-pace interspersed to maintain good running form. When training for my first a marathon after not running at all for two years (the typical first marathon experience), I developed a good deal of kneecap pain on both sides about two months into regular training. I spent the next 14 weeks doing one long run every 8-10 days and one short run a week. Every other training day I spent on the elliptical and in the weight room, and ended up beating my time goal for the race by ten minutes. Interval training can also be very effective. The change in mechanics from running/jogging to sprinting can alter the forces enough to make very high-intensity training pain-free. The numbers will vary by event and athlete, but try sprinting for 10-20 seconds, resting for 10-20, and repeating for 4-6 minutes, followed by walking/active rest. Repeat, using total time, rather than distance, as your guide. You may also try integrating lower-intensity agility exercises into your program. Backwards jogging, side-shuffles, cariocas, skipping, heel kicks and other exercises are good ways to break up the monotony of running and alter the stresses on the kneecap.

Or break up the monotony of running by climbing up ropes and over fences, swimming through mudholes and running through fire. Just a thought.
All of the above are ways to minimize stresses. Decreasing inflammation is also important. I generally recommend ice after activity, at least 10 minutes and no more than 20 minutes at a time. Icing multiple times throughout the day is probably better, though this is likely subject to the law of diminishing returns: icing three times a day is better than once, but is it three times better? Probably not. Do what you can. You may also consider talking with your doctor about taking an over the counter anti-inflammatory such as Advil or Aleve as a short-term solution.
So far we have dealt with ways to minimize pain, but what about addressing the causes? Despite there being a lot of research, and a whole lot of things that correlate with increased incidence of kneecap pain (tight hamstrings, weak quads, tight ITB, weak hamstrings, overpronation, weak glutes, an increased Q-angle, and poor core stability are all risk factors for increased pain in and around the kneecap), there is less evidence to show that a specific intervention (ie, foam rolling your ITB or doing quadricep exercises) fixes everyone who tries them. The reason for this is precisely that there are so many possible--and overlapping--causes, and when doing academic studies it is nearly impossible for researchers to create a study with sufficient subjects with the same objective cause of the kneecap pain. This underscores the need to seek out the expertise of a sports medicine specialist (even if you are not an athlete) when dealing with kneecap pain that has lasted longer than 1-2 weeks or is time-sensitive due to an upcoming event such as travel or a race. In most cases the best option is a Physical Therapist who focuses on orthopedic issues, who will perform a full evaluation on the trunk and lower extremity, diagnose the causative factors, and design a plan of care to rectify them. A Medical Doctor who has completed an orthopedic surgery or sports medicine fellowship is also a good choice, but in most cases, due to constraints on their time, they will make the diagnosis of Patellofemoral Pain and then refer the patient out to a Physical Therapist for evaluation and treatment of the causes. By seeing a Physical Therapist first the start of care is not delayed, and if a referral is needed to a Physician (for drugs, injections, or a surgical evaluation), a very strong clinical basis for medical care will have already been established.

We'll all eventually have to switch to Power Walking, but follow the advice above, and it might not be till you're 90.